Meningitis, a formidable and potentially devastating inflammation of the protective membranes encasing the brain and spinal cord, demands immediate recognition and intervention, with vaccination representing a cornerstone of public health defense against its most dangerous forms. Recent health alerts underscore the critical importance of understanding this infection, its varied manifestations, and the comprehensive strategies available for prevention and treatment.
Heightened Vigilance Following Regional Health Incidents
The recent confirmation of multiple fatalities and a cluster of cases involving meningococcal disease in the Canterbury area of the United Kingdom has prompted an urgent public health response and intensified community concern. Two young individuals, one a student at Queen Elizabeth’s Grammar School in Faversham and another enrolled at the University of Kent, tragically succumbed to the illness. This cluster, which saw the UK Health Security Agency (UKHSA) notified of thirteen presumptive cases exhibiting symptoms of meningitis and septicaemia within a concentrated period, has galvanized extensive preventative measures. Public health authorities are proactively distributing antibiotics to specific segments of the student population as a precautionary measure, aiming to interrupt any potential spread. Furthermore, an expansive communication initiative is underway, targeting over 30,000 students, staff, and their families within the Canterbury region to disseminate vital information and guidance. This coordinated effort highlights the rapid and decisive action required to mitigate the impact of such severe infectious disease outbreaks in densely populated educational environments.
Dissecting Meningitis: A Critical Overview
Meningitis fundamentally involves the inflammation of the meninges—the three layers of protective membranes (dura mater, arachnoid mater, and pia mater) that surround the brain and spinal cord. This inflammation can result from various etiologies, predominantly bacterial or viral infections, though fungal and parasitic causes are also possible, albeit less common in developed nations. While anyone can contract meningitis, specific demographics, including infants, young children, adolescents, and young adults, exhibit a higher susceptibility, often due to their developing immune systems or close communal living arrangements. The gravity of meningitis cannot be overstated; prompt diagnosis and treatment are paramount, as delays can lead to severe, irreversible neurological damage or prove fatal.
The distinction between bacterial and viral meningitis is crucial due to significant differences in severity and treatment. Viral meningitis, though often presenting with similar symptoms, is generally less severe and typically resolves without specific intervention, requiring only supportive care. In contrast, bacterial meningitis is a medical emergency. It is rarer but far more aggressive, capable of causing life-threatening complications, including brain damage, hearing loss, learning disabilities, and limb amputation, even with optimal treatment. The most perilous manifestation of bacterial meningitis is "invasive meningococcal disease," which signifies that the causative bacteria have not only infiltrated the meninges but have also breached the bloodstream, leading to septicaemia, or blood poisoning. This acute, severe form of the disease progresses rapidly, overwhelming the body’s defenses and often resulting in a distinctive rash. The two individuals who died in the Kent outbreak were reportedly between 18 and 21 years old, an age group particularly vulnerable to meningococcal disease, though the precise bacterial strain responsible for the recent cluster remains under active investigation.

Recognizing the Alarming Indicators: Symptoms and Progression
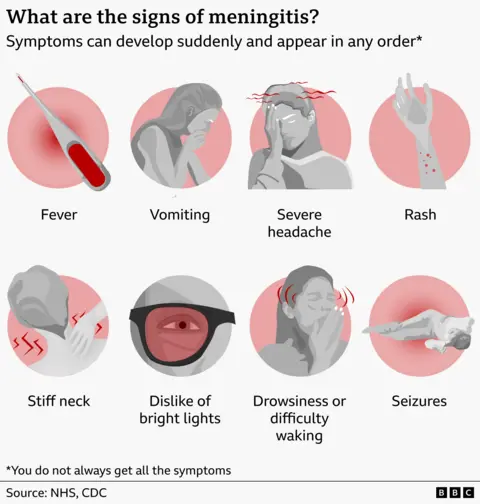
The symptoms of meningitis can emerge abruptly and escalate with frightening speed, making early recognition a critical factor in patient outcomes. Common indicators often include a high fever, accompanied by chills and sometimes shivering, and persistent vomiting. A hallmark symptom is a severe headache, often described as throbbing or unremitting, distinct from a typical tension headache. Stiffness in the neck, which can make it difficult or painful to touch the chin to the chest, is another key sign. Sensitivity to bright lights (photophobia) is also frequently reported. Patients may experience unusual drowsiness, confusion, or difficulty waking, indicating neurological compromise. In some severe cases, seizures may occur.
One of the most concerning and urgent signs, particularly in cases of meningococcal septicaemia, is the development of a rash. This rash typically begins as tiny red or brown pinprick spots that, unlike many other rashes, do not fade or blanch when a glass is pressed firmly against them. As the disease progresses, these spots can enlarge into larger red or purple blotches, resembling bruises. On individuals with darker skin tones, this rash may be less obvious and should be checked on paler areas such as the palms of the hands, soles of the feet, the roof of the mouth, or inside the eyelids. The appearance of such a non-blanching rash is a medical emergency and necessitates immediate professional medical attention. It is crucial to remember that not all symptoms may present simultaneously, and waiting for all signs or the rash to appear can be a fatal delay.
Understanding Transmission Patterns
Meningitis-causing bacteria and viruses are typically transmitted through respiratory droplets and close, prolonged contact with an infected individual. Many people can carry these bacteria, particularly Neisseria meningitidis (which causes meningococcal meningitis), in their nose or throat without developing any symptoms themselves. These asymptomatic carriers can, however, unknowingly transmit the bacteria to others through activities that involve the exchange of respiratory secretions, such as coughing, sneezing, kissing, or sharing eating utensils, drinks, or cigarettes. While transmission from someone who is actively ill with meningitis is possible, it is less common than from asymptomatic carriers. Importantly, an individual can contract meningitis more than once, especially if different strains or types of pathogens are involved.
The recent outbreak in Kent is reportedly linked to a social gathering in Canterbury, underscoring a well-documented epidemiological pattern: outbreaks of meningococcal disease are more prone to occur in settings where people live or congregate closely, such as college dormitories, military barracks, or boarding schools. These environments facilitate the rapid spread of respiratory pathogens among a susceptible population, making communal living a recognized risk factor for meningococcal disease. Understanding these transmission dynamics is vital for implementing effective public health interventions like contact tracing and targeted prophylactic treatments.
Mitigation and Prevention: The Role of Antibiotics and Vaccines

Controlling the spread of meningococcal disease, particularly during an outbreak, hinges on swift and decisive public health measures. A primary strategy involves the administration of prophylactic antibiotics to individuals who have had close contact with a confirmed case. This "post-exposure prophylaxis" aims to eradicate the bacteria from the carrier’s nose and throat, thereby preventing them from developing the disease or transmitting it further. This is precisely the rationale behind the precautionary antibiotic distribution to students in the Canterbury area, even as the specific strain of the invasive meningococcal disease is being identified.
The most powerful long-term defense against meningitis, however, lies in vaccination. Several vaccines provide targeted protection against the major causative agents of meningitis and septicaemia:
- MenACWY Vaccine: This vaccine offers protection against four specific serogroups of Neisseria meningitidis—A, C, W, and Y. It is routinely offered to adolescents around 14 years of age in many national immunization programs, recognizing this age group’s increased risk and potential role in transmission.
- MenB Vaccine: Targeting meningococcal group B bacteria, which is a common cause of bacterial meningitis in infants, the MenB vaccine is typically incorporated into early childhood immunization schedules. Babies usually receive their first dose at eight weeks, followed by a second dose at 12 weeks, and a booster around one year of age.
Beyond these specific meningococcal vaccines, several other routine immunizations indirectly contribute to meningitis prevention by protecting against infections that can sometimes lead to meningitis as a complication:
- DTaP/IPV/Hib/Hep B (Six-in-One) Vaccine: Administered to young children, this vaccine protects against Haemophilus influenzae type b (Hib), which was once a leading cause of bacterial meningitis before the introduction of widespread vaccination.
- Pneumococcal Vaccine: This vaccine protects against serious infections caused by Streptococcus pneumoniae, including pneumococcal meningitis, another significant cause of bacterial meningitis, particularly in young children and the elderly.
- MMRV Vaccine: Given to infants, this vaccine protects against measles, mumps, rubella, and chickenpox. While less direct, these viral infections can sometimes lead to viral meningitis or encephalitis.
It is important to note that full immunological protection from vaccines typically takes a few weeks to develop, and some vaccines necessitate booster doses to ensure sustained immunity. The success of these vaccination programs has dramatically reduced the incidence of several types of meningitis, transforming the landscape of pediatric infectious diseases.
Assessing Immunization Status and Addressing Coverage Gaps
Maintaining up-to-date vaccination records is paramount for individuals and public health alike. Individuals unsure of their vaccination history should consult their general practitioner or review personal health records, such as the "red book" commonly used for childhood immunization records in the UK. A significant concern in recent years has been a decline in vaccine coverage, exacerbated by factors such as the COVID-19 pandemic, leading to a greater proportion of the population being unprotected against preventable diseases.
To address these gaps, catch-up programs are often in place. For instance, the MenACWY vaccine is typically offered free of charge to anyone who missed their scheduled dose at school, up to their 25th birthday. Similarly, the MMR vaccine is universally free for individuals of any age who missed it during childhood. However, the MenB vaccine presents a more complex public health policy challenge. While introduced into the UK childhood immunization program for babies born on or after July 1, 2015, it is not routinely offered as a catch-up vaccine for adolescents or young adults.
The decision not to extend the MenB vaccine to older age groups on the National Health Service is rooted in a multifaceted assessment by vaccine experts. Research indicates that the MenB vaccine’s impact on reducing the transmission of the infection from person to person is limited. Furthermore, the vaccine does not protect against all existing group B bacterial strains and its protective effects may not be particularly long-lasting in adolescents. Given these factors, coupled with the higher incidence and greater vulnerability of young babies to invasive meningococcal B infections, vaccine experts have concluded that a widespread MenB vaccination program for adolescents is not currently deemed cost-effective for the NHS, despite persistent advocacy from charities and patient groups. This policy underscores the complex balance between individual protection, population-level impact, and resource allocation in public health.
Immediate Action: A Critical Imperative
In the event that an individual, or someone they are with, begins to exhibit symptoms suggestive of meningitis or septicaemia, immediate medical attention is non-negotiable. Dialing emergency services (e.g., 999 in the UK) or proceeding directly to the nearest Accident and Emergency Department can be life-saving. Early treatment, typically involving intravenous antibiotics for suspected bacterial meningitis, significantly improves prognosis.
Public health officials consistently advise at-risk populations, particularly students living in communal settings, to trust their instincts and not delay seeking help. The early warning signs of meningitis can be deceptively similar to less serious conditions like a common cold, influenza, or even a hangover. This potential for misinterpretation makes vigilance even more crucial. Students are urged to check on friends who may be feeling unwell and to seek professional medical advice without hesitation, whether through emergency services, a general practitioner, or a non-emergency medical helpline. Prompt action can differentiate between a full recovery and severe, irreversible consequences.
In conclusion, while meningitis remains a serious public health threat, particularly in specific age groups and communal environments, comprehensive vaccination programs and robust public health response protocols offer substantial protection. Continued public awareness of symptoms, coupled with adherence to recommended immunization schedules and immediate medical consultation when symptoms arise, are collectively vital in mitigating the impact of this challenging disease.